Myocardial Infarction Explained

An In-Depth look: From Chest Pain to STEMI, EKG Changes, Troponin, and Opening the Blocked Artery
The Biology of a Blocked Artery
Chest pain is one of the most common reasons patients come to the emergency department. Among the many possible causes, myocardial infarction is one of the most time-sensitive and potentially life-threatening. Understanding how it develops, how it appears on the EKG, and how it is treated requires understanding the biology happening beneath the symptom.
A heart attack is not simply pain. It is a process.
What a Heart Attack Actually Is
The medical term for heart attack is myocardial infarction. Myocardial means heart muscle. Infarction means tissue death. A heart attack is death of heart muscle caused by sudden loss of blood flow.
The heart is a muscle that never rests. To keep pumping, it needs its own blood supply through coronary arteries. Over time, cholesterol rich plaques can build inside those arteries. If a plaque ruptures, a blood clot forms on top of it. That clot can completely block the artery. When blood stops flowing, oxygen delivery stops. Within minutes, heart muscle cells begin to die.
What the EKG Is Really Showing
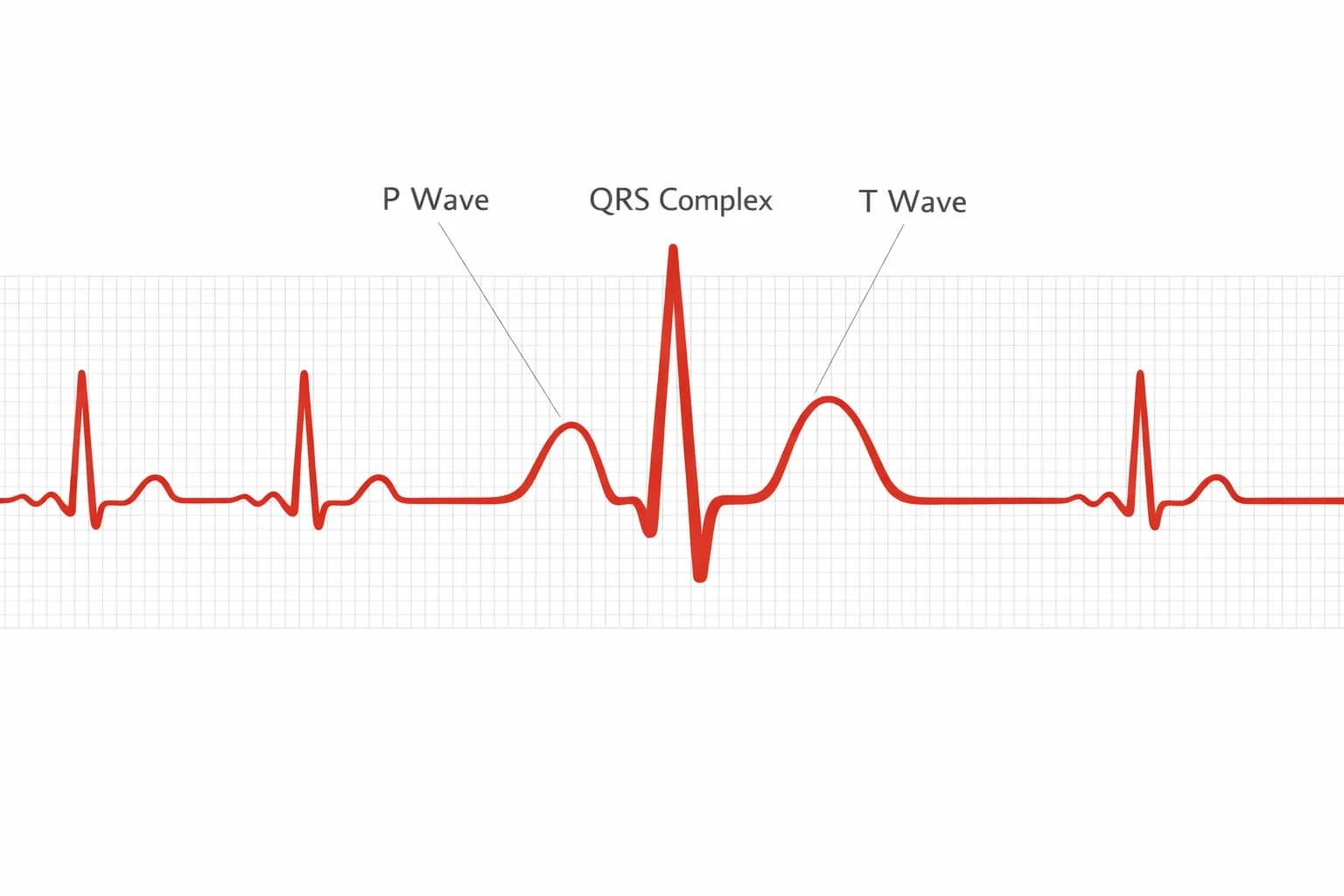
An electrocardiogram, or EKG, records the electrical activity of the heart. Each heartbeat begins with an electrical impulse that travels through the muscle and causes it to contract. On the tracing, the P wave represents atrial contraction. The QRS complex represents ventricular contraction. The ST segment is the flat portion immediately after the ventricles contract and before they reset for the next beat. Under normal conditions, the ST segment sits on the baseline. Quiet. Neutral.
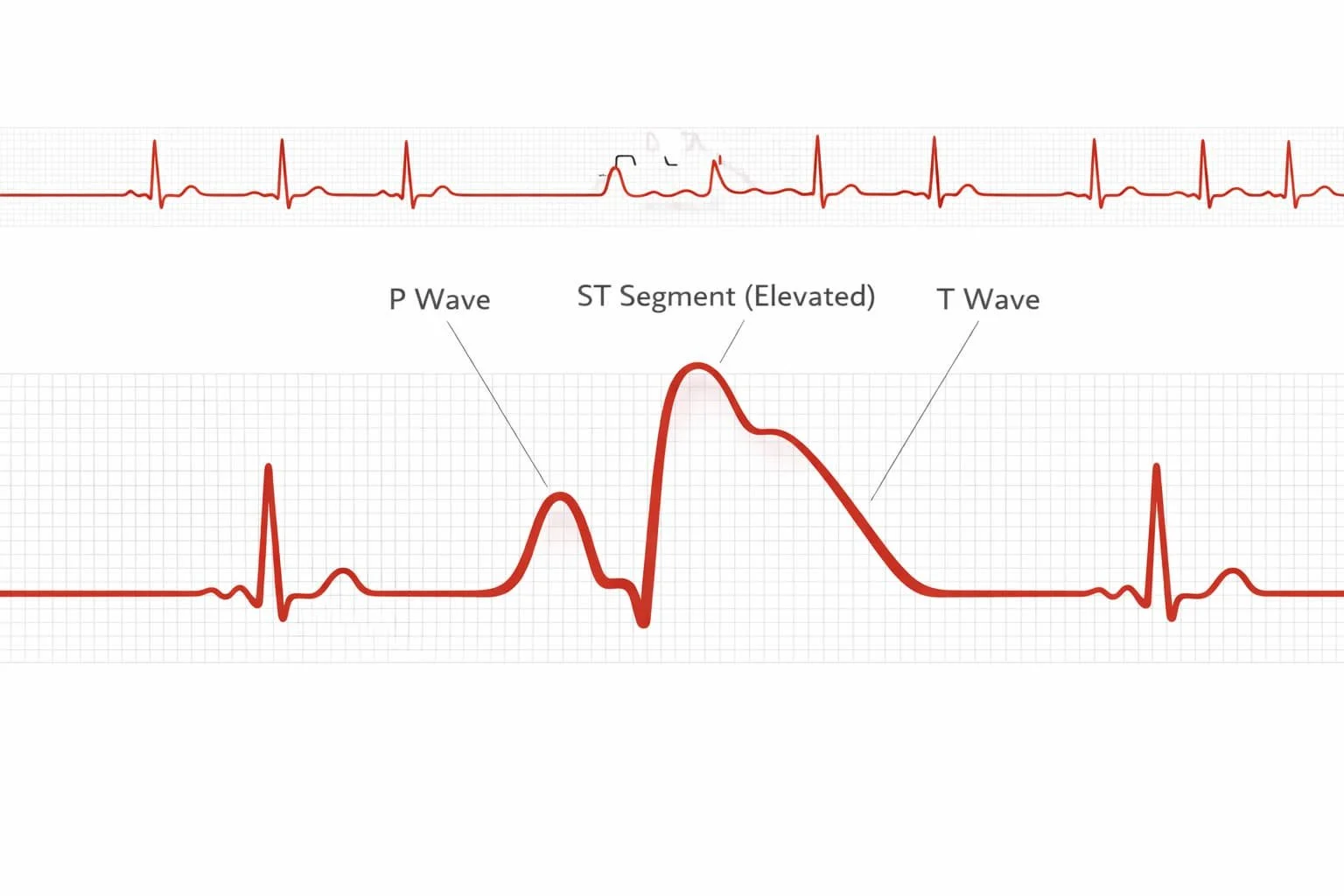
When a coronary artery suddenly becomes blocked, the affected heart muscle becomes ischemic, meaning deprived of oxygen. If that deprivation involves the full thickness of the muscle wall, the electrical properties change. The ST segment rises above the baseline. This is called ST elevation.
ST elevation myocardial infarction, or STEMI, signals that an artery is likely completely blocked at that moment. The EKG does not show the clot directly. It shows the electrical consequence of muscle that is starving. That is why when we see ST elevation, the cath lab is activated immediately.
Not All Heart Attacks Look the Same
Some heart attacks do not show ST elevation. The artery may be partially blocked or intermittently occluded. The EKG may show ST depression or T wave inversion instead. The T wave represents ventricular recovery after contraction. When it flips or changes shape, it can signal ischemia.
In those cases, blood tests become crucial. Troponin is a protein released into the bloodstream when heart muscle cells are injured. Elevated troponin confirms myocardial damage even if the EKG is subtle. These are called NSTEMIs, non ST elevation myocardial infarctions. They are serious and require hospitalization, but they may not demand the same immediate door to balloon activation as a STEMI. Women and diabetic patients often present differently. They may not describe crushing chest pain. They may report shortness of breath, fatigue, nausea, or back discomfort. That is why we do not rely on one textbook description.
Time Is Muscle
When a coronary artery closes, every minute matters. The longer heart muscle is deprived of oxygen, the more tissue dies. Dead muscle does not contract. It does not recover.
Modern systems aim for door to balloon time under ninety minutes. That means from arrival at the emergency department to inflation of a balloon in the blocked artery in the cardiac catheterization lab. During those minutes we give aspirin, usually 324 milligrams, because aspirin prevents platelets from worsening the clot. We may give heparin, a blood thinner that reduces further clot formation.
Nitroglycerin can improve blood flow and relieve pain, though it must be used carefully in certain types of heart attack that affect the right ventricle. Pain relief is important. Opening the artery is everything.
Opening the Artery
Definitive treatment in most modern centers is emergent cardiac catheterization. A cardiologist threads a thin catheter through an artery in the wrist or groin and guides it to the coronary arteries using fluoroscopy, which is real time X ray imaging. Contrast dye outlines the vessels. The blockage becomes visible.
A balloon is inflated to reopen the artery. A stent, a small metal scaffold, is placed to keep it open. Blood flow returns. When done quickly, this restores oxygen delivery and limits permanent damage. In areas without immediate access to a cath lab, clot dissolving medications such as tenecteplase may be used. They can be lifesaving but carry bleeding risks and are less precise than direct mechanical opening.
It Is Not Always Heartburn
Many patients arrive saying it is probably just indigestion. Sometimes it is. Sometimes it is not.
Severe reflux can mimic heart attack. So can pulmonary embolism or aortic dissection. That is why we evaluate carefully before giving powerful blood thinners. But when chest pain is new, severe, pressure like, associated with sweating or shortness of breath, it is not the moment for denial. The heart does not reward hesitation.
THE BOTTOM LINE
• A heart attack, or myocardial infarction, is death of heart muscle caused by sudden blockage of a coronary artery
• Classic symptoms include crushing chest pain, sweating, and shortness of breath, but women and diabetics may present atypically
• Rapid treatment with aspirin and emergency cardiac catheterization saves heart muscle and lives
By Dr. Karim Ali, Emergency Physician